
KUALA LUMPUR, Sept 11 – Despite implementing various policies to address sexual and reproductive health education among young Malaysians, less than 60 per cent of adolescents in the country have basic knowledge of sexual reproductive organs, according to the UNFPA report Enhancing Human Capital through Sexual and Reproductive Health Investment and Family Support Policies in Malaysia.
The level of knowledge regarding sexual intercourse is even lower.
Based on the report, 7.3 per cent of 13 to 17-year-olds surveyed in 2017 said that they have engaged in sexual intercourse, and less than one-third used condoms or some other form of birth control.
Comprehensive Sexuality Education (CSE) for adolescents helps prevent teen pregnancies as well as HIV and other sexually transmitted infections (STIs), deterring students from dropping out of school and enabling them to avoid poverty by enhancing lifetime earnings and general well-being, according to the report.
In 2018, the adolescent birth rate was estimated at 8.8 births per 1,000 women aged 15 to 19 years. Furthermore, 15,000 cases of child marriage was recorded the same year, with an estimated 100 cases of baby dumping discovered annually since 2008.
‘Reproductive Health’ Not Accepted, ‘Sexual Health’ Even More Controversial

Dr Raj Karim, vice-president of the Federation of Reproductive Health Association, Malaysia, recalls a time not too far back when the term Sexual and Reproductive Health was met with disapproval.
“UNFPA will probably remember at the time (1994), the words ‘reproductive health’ was not accepted, ‘sexual health’ was even more controversial,” she said during a panel discussion at the launch of the report last July.
The International Conference on Population Development (ICPD), which resulted in the Cairo Plan of Action that year was a milestone, as it introduced the terminology Sexual and Reproductive Health (SRH), said Dr Raj who has been a sexual and reproductive health and rights (SRHR) advocate in Malaysia for 51 years.
Gaping Deficit In Sexual And Reproductive Health Knowledge Among Youths
While Malaysia has implemented a number of policies including the National Policy in Reproductive Health and Social Education (PEKERTI) and Plan of Action, as well as the Sexual and Reproductive Health Education (PEERS), which focuses on reproductive health and CSE, more must be done to address the gaping deficit in sexual and reproductive health knowledge among youths, as reflected in the survey and figures.
According to the UNFPA report, the success of CSE programmes in Malaysia can be strategically improved by addressing a number of factors including:
- Cultural sensitivity and understanding around the impacts of CSE.
- Consensus on a national curriculum.
- Consistency in skills and attitudes of teachers and trainers.
- Increased family and parental buy-in and involvement.
- Effective collaboration among stakeholders.
- Sustainable, targeted funding for CSE design, implementation and evaluation.
CSE must be “medically accurate, evidence-based, and age-appropriate, and should include the benefits of delaying sexual intercourse, while also providing information about normal reproductive development, contraception to prevent unintended pregnancies, as well as barrier protection to prevent STIs,” the report maintains.
It has proven to be very effective at reducing the number of unintended pregnancies and STIs among adolescents, including HIV and HPV.
Since adolescent pregnancies are at increased risk of unsafe abortions and adverse maternal, perinatal and infant outcomes, CSE yields direct health benefits by preventing mortality and morbidity impacts associated with adolescent pregnancy and STI.
In addition, unintended adolescent pregnancies are associated with decreased educational attainment. The UNFPA’s empirical analysis found that, among the respondents to the Fifth Malaysian Population and Family Survey, the risk of not completing secondary education is three times greater among girls with an adolescent pregnancy compared to women who had their first pregnancy after age 20.
Given the high schooling return rates in Malaysia, especially for women, low educational attainment has lifetime negative consequences.
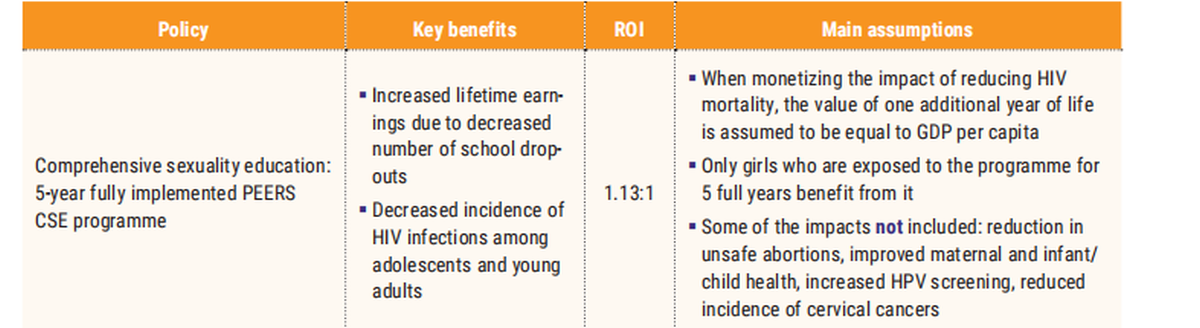
As such, in calculating the ROI for CSE, the UNFPA focused on two positive outcomes of CSE, namely increased lifetime earnings due to decreased number of school dropouts, and decreased incidence of HIV infections.
However, this computation excludes other benefits such as reduced incidence of other STIs, and improved maternal and child health from preventing high-risk adolescent pregnancies.
ROI Through Prevention Of Loss Of Lifetime Earnings

An estimated 12,944 adolescent pregnancies were recorded in 2017, including 12,748 live births, 96 stillbirths, and 100 cases of “baby dumping” (for adolescents aged 10 to 19 years), according to the report, which also notes that miscarriage and abortion rates among adolescents are currently unknown, indicating that the number of adolescent pregnancies is underestimated.
While there are no figures for how many of these pregnancies and births are unintended, the Demographic and Health Survey reports that the percentage of unintended births among adolescents in Southeast Asia is, on average, 13.8 per cent, notes the UNFPA report.
Based on this number, roughly 1,800 births (13.8 per cent x 12,944) among adolescents are estimated to be unintended. This can be considered the lower bound in the number of unintended births among adolescents.
Taking into account an estimated 4,500 pregnancies each year that are reported to be out of wedlock and assuming that all these pregnancies end in an unintended birth, the (conservative) upper bound in the number of unintended births among adolescents is 5,600 (44.2 per cent).
As such, the UNFPA report estimates that annually about 1,800 to 5,600 births among adolescents are unintended (an average of 3,700 births).
Based on average measures of CSE effectiveness from developed countries, the UNFPA report maintains that a minimum of five years of exposure to CSE can reduce unintended adolescent pregnancies by 49 per cent, which means that approximately 1,800 live births from unintended pregnancies could be averted through CSE (i.e. between 870 and 2,700).
This is the reduction in unintended births if one birth cohort of adolescent girls is exposed to a five-year, fully implemented CSE programme, assuming that only full attendance to the programme will be effective at reducing the number of adolescent pregnancies.
The UNFPA employs the returns to schooling estimates from the World Bank study (where the returns from an additional year of schooling are 13.8 per cent for women), in its calculations, determining that one year of decreased educational attainment can lead to an average decrease in discounted lifetime earnings of roughly RM120,000 (discounted at a rate of 3.0 per cent).
Assuming that each woman with an unintended adolescent birth loses one year of schooling, an effective CSE programme can prevent total lost lifetime earnings of roughly RM215,834,000 (i.e. between RM104,841,000 and RM326,171,900), notes the report.
Sexual Activity Main Cause Of HIV Infection
While the UNFPA’s calculations exclude other STIs, Dr Raj says the focus on STDs has to be looked at within the context of HIV: “Because I read another report that shows that if you ask adolescents about STDs, more of them do not know what gonorrhoea, syphilis, or chlamydia is, but they know HIV/AIDs.”
“So, the knowledge gap is big. And if you look at the issues facing youth today, to me it’s like a three-in-one. It is teenage pregnancy, it is HIV/AIDS, and it is also drug abuse that goes hand-in-hand.
Dr Raj Karim
“We need to look at the awareness, social media, peer pressure and all the other factors that precipitate the increase in STDs among youths. The rate of HIV now is highest among the youth, and sexual activity has taken over (as the main cause of HIV infection in the country) from intravenous drug use,” said Dr Raj.
The UNFPA report confirms that approximately 95 per cent of new HIV infections are sexually transmitted and more than 70 per cent of new HIV infections are among people aged 20 to 39.
Currently, the HIV incidence rate in Malaysia is around 0.17 to 0.20 per 1,000 people, and has remained constant over the last ten years.
Life expectancy among HIV-positive individuals has increased over the years thanks to improved treatments, often reaching levels close to the general population.
The Global Burden of Disease estimates that in Malaysia, HIV results in 6,364.29 years lived with disability (2019 estimate).
Given that 77,903 individuals are currently living with HIV, the average years lived with disability per person associated with HIV are 0.082 (i.e. HIV-positive persons live on average 8.2 per cent of their life years with a disability).
This loss in health is due to other conditions that result from HIV, such mycobacterial infection or AIDS.
Assuming that the average age of HIV infection is 25 years old, and that, optimistically, the life expectancy of an HIV-positive person is 10 per cent lower than the life expectancy of the rest of the population, HIV-positive individuals lose about 7.5 years of life (68.30 versus 75.83), and live 8.2 per cent of the rest of their life (i.e. 43.3 years) with a disability.
This results in a burden of disease of 11 disability-adjusted life years (DALYs) per person, where the number is obtained by summing the years of life lost (7.5) and the years lived with a disability (43.3 years).
Monetising The Burden Of Disease From HIV
The UNFPA uses the value of statistical life method to monetise the burden of disease due to HIV, which is measured using the value of statistical life year (VSLY) concept.
The VSLY represents the amount of money an individual is willing to sacrifice for an additional year of life and is generally assumed to be one to three times income per capita.
With a gross domestic product (GDP) per capita of RM46,450, (based on the Department of Statistics Malaysia State Socioeconomic Report 2019-2020), one averted case of HIV is valued between RM516,953 and RM1,550,800, where the numbers have been computed by multiplying the DALYs per person associated with HIV by the VSLY.
Referencing average measures of CSE effectiveness from literature, the UNFPA report assumes that a five-year exposure to CSE in Malaysia is 62 per cent effective at averting new HIV infections.
Based on current incidence rates, the yearly HIV incidence rate for the rest of the population is estimated to be 0.17 per 1,000, while the yearly incidence rate for the birth cohort exposed to the full CSE programme is 62 per cent lower (0.07 per 1,000.)
On the assumption that the programme is effective at reducing the incidence rate of HIV for adolescents and young adults (ages 15 to 29) — while neglecting the longer-term effects due to uncertainty over the HIV incidence rate in the future — for a birth cohort reaching adolescent age, the risk of contracting an HIV infection before age 30 is approximately equal to 0.25 per cent.
This number accounts for the yearly HIV incidence rate of 0.17 per 1,000, and for the population survival curve between ages 15 and 30. Given that the size of one birth cohort reaching adolescent age is about 522,000 people, roughly 1,300 of them are expected to be infected with HIV before age 30.
Value Of CSE Programme
Exposure to the CSE programme can reduce the incidence of HIV by 823 cases. Multiplying by the monetary value of one averted case of HIV (between RM516,953 and RM1,550,800), the total value of the programme for one cohort is between RM425,519,800 and RM1,276,559,600.
Considering both the gains in lifetime earnings due to increased years of schooling, that would otherwise be lost due to teenage pregnancy, and the decrease in DALYs due to lower HIV prevalence, lifetime benefits for a single birth cohort resulting from investing in CSE are estimated to be RM641,353,900 if the VSLY is valued at GDP per capita (or RM135 per student), and RM1,492,393,600 if the VSLY is valued at three times GDP per capita (or RM315 per student).
The UNFPA employs the Ministry of Education budget data to estimate the cost of a five-year, fully implemented PEERS CSE programme. Training is estimated to cost RM4,000 per trainer/teacher.
Assuming that all 10,208 primary and secondary schools will have at least two trained teachers to deliver the PEERS curriculum each year, a one-time training cost for a five-year period and teacher salary for 22 hours per class (16 hours in-class time and six hours of teacher preparation time per class) were also factored in.
The costs of the universal five-year CSE programme across all primary and secondary public schools in Malaysia are estimated to be RM565,505,049 million, which translates to RM119 per student for all five years, according to the report.
Given the estimated benefits and costs, the ROI for fully investing in universal CSE for a five-year period is on average 13 per cent (1.13:1) if one year of life is valued at GDP per capita; it increases to 264 per cent (2.64:1) if one year of life is valued at three times GDP per capita.
Despite the potential benefits of the PEERS CSE curriculum, funding dropped by a factor of 10 over the past five years (from RM120,000 in 2015 to RM12,000 in 2019), the report noted.
CSE Not Just For Young People

Dr Subatra Jayaraj, president of the Reproductive Rights Advocacy Alliance Malaysia (RRAAM), said CSE should not be limited to just young people. “Definitely CSE should be at the core because it has been proven to improve reproductive health throughout the life cycle. But somehow, when we talk about CSE, it’s always related to young people. And then it becomes a deflection of blame.
“Every three days one baby is dumped in Malaysia. We seem to deflect it to that young unfortunate pregnant woman who is caught just because she’s in a vulnerable position in society. I have never seen any high-quality data that relates teenage pregnancies to baby dumping,” said Dr Subatra, who was also a panellist during the launch.
“Our teenage pregnancy rates have come down from about 18,000 to 10,000 to 12,000. But still we shift the blame to young people because of our investment in SRH at every level. So, everytime a baby is dumped, I say it is a failure of the system. It’s a failure of governments, health providers, schools, head of households and we are not recognising that.”
Dr Subatra said primary prevention of unintended pregnancies through CSE should be invested in for everyone. Secondary prevention comes in the form of universal access to high quality contraception care.
“We’ve seen how it works in Malaysia. We seem to think only certain populations have sex. And this is a policy issue, it’s not an individual issue.”
“Tertiary prevention for unintended pregnancies are early options for termination of pregnancy, which have been available since 1989 for all pregnant persons up to 22 weeks,” Dr Subatra continued, adding that socio-religious stigma prevents women from accessing this prevention option.
“Finally, if we fail this pregnant person for so long; at all these three steps, if a person has an unintended pregnancy at an advanced gestation, we need (to provide them with) good social support. But that social support needs to be non-judgemental, non-discriminatory, and non-punitive.
“We have senators asking in Parliament about illegitimate children. What the hell are ‘illegitimate children’?”
Dr Subatra Jayaraj
“So we need to ask ourselves, every time a baby is dumped, are we going to blame that young teenage person who was only unfortunate to get caught? Or are we going to blame our lack of addressing these social, religious, political and religious barriers, and not investing enough in CSE? Or just carry on?
“We cannot just carry on. We have a lot of data, we need to invest in proven strategies that work.”


